By Peter H. Langsjoen, MD STATIN-INDUCED CARDIOMYOPATHY
Dr Langsjoen has a paper on the FDA website about statins reducing serum levels of CoQ10.
"The medical profession has, after more than 30 years of excellent propaganda, successfully created the wholly iatrogenic - "pseudo-disease" dubbed "hypercholesterolemia" and the associated malady "cholesterol neurosis". After decades of dismal failure to cure this "disease" of numbers with low fat diets and a host of cholesterol lowering drugs, the medical profession stumbled upon the magic bullet, the cure for this dreaded artificial disease - statins (HMG-CoA reductase inhibitors). First released on the US market in 1987, statins have rapidly grown into one of the most widely prescribed class of drugs in history. Statins do three things:
1. They block the body's ability to make cholesterol, thus lowering the blood level of cholesterol, thereby curing cholesterol neurosis. Doctors and patients equally neurotic have immediate gratification. The "evil" high cholesterol has been dramatically lowered and the future is bright and promising. So far...so good.
2. Unrelated to their cholesterol lowering, statins have been found to have anti-inflammatory, plaque-stabilizing properties which have a slight benefit in coronary heart disease.
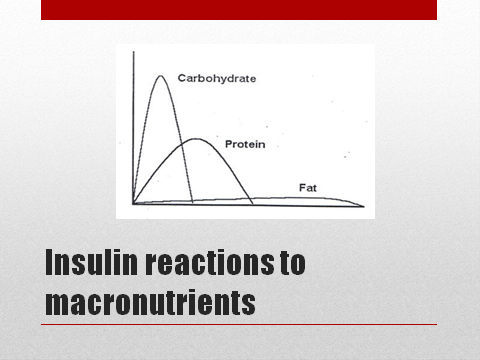
3. Statins kill people - lots of people - and they wound many, many more. All patients taking statins become depleted in Coenzyme Q10 (CoQ10), eventually - those patients who start with a relatively low CoQ10 levels (the elderly and patients with heart failure) begin to manifest signs/symptoms of CoQ10 deficiency relatively rapidly - in 6 to 12 months. Younger, healthier people who's only "illness" is the non-illness "hypercholesterolemia" can tolerate statins for several years before getting into trouble with fatigue, muscle weakness and soreness (usually with normal muscle enzyme CPK tests) and most ominously - heart failure.
In my practice of 17 years in Tyler, Texas, I have seen a frightening increase in heart failure secondary to statin usage, "statin cardiomyopathy". Over the past five years, statins have become more potent, are being prescribed in higher doses, and are being used with reckless abandon in the elderly and in patients with "normal" cholesterol levels. We are in the midst of a CHF epidemic in the US with a dramatic increase over the past decade. Are we causing this epidemic through our zealous use of statins? In large part I think the answer is yes.
We are now in a position to witness the unfolding of the greatest medical tragedy of all time - never before in history has the medical establishment knowingly (Merck & Co., Inc. has two 1990 patents combining CoQ10 with statins to prevent CoQ10 depletion and attendant side effects) created a life threatening nutrient deficiency in millions of otherwise healthy people, only to then sit back with arrogance and horrific irresponsibility and watch to see what happens - as I see two to three new statin cardiomyopathies per week in my practice, I cannot help but view my once great profession with a mixture of sorrow and contempt."
More on this article from July 8, 2002 here. With NICE pushing for millions more adults to be on statins in the UK, will they be recommending Coenzyme Q10 supplementation for statin users ? probably not, it's all down to cost you see. We want you on statins, but please don't ask for Coenzyme Q10, the budget doesn't run that high, on your way lad, next patient please !
Eddie (my bold text)